7-year-old male German Pointer presented for chronic non-ambulatory tetraparesis, with increased reflexes of the pelvic limbs and decreased reflexes in thoracic limbs. An MRI scan of the cervical spine was performed.
Description
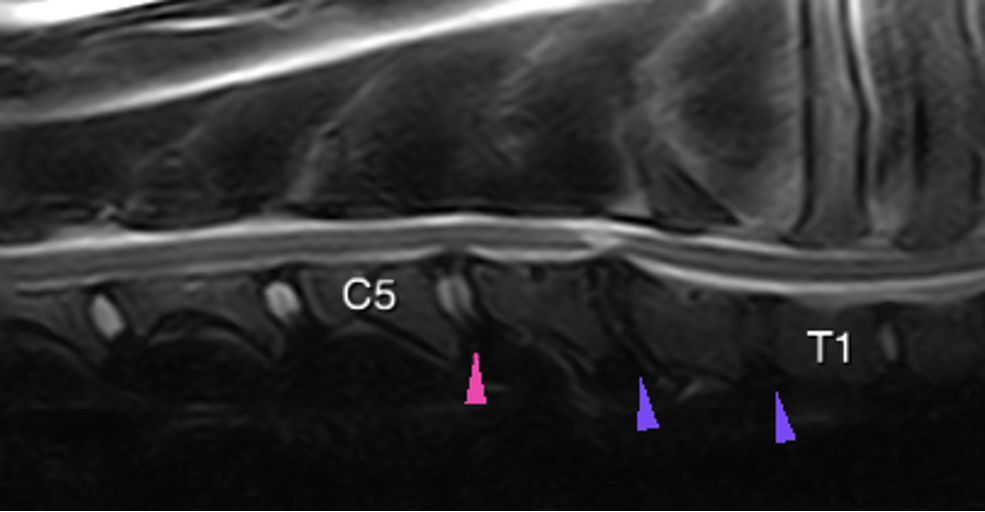
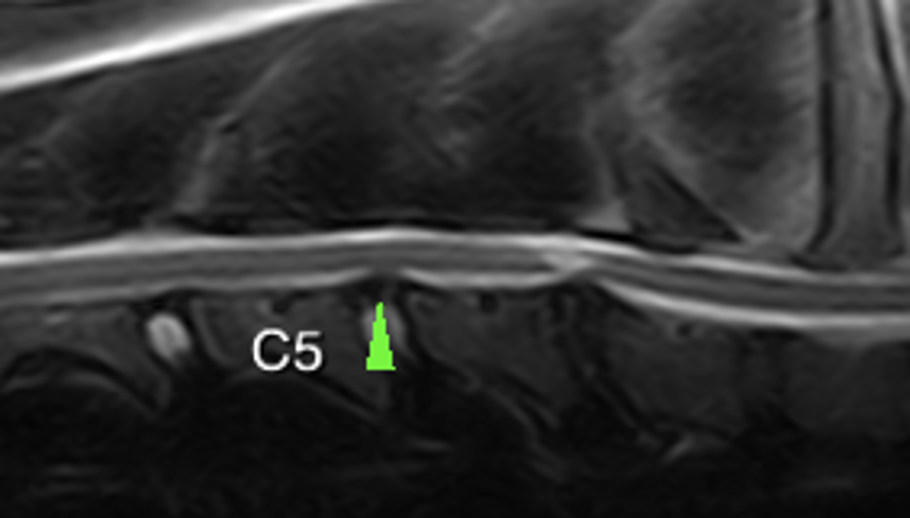
The IV disc of C5-C6 shows a decreased hyperintense signal (pink arrowhead) and the IV discs of C6-T1 are hypointense on T2W (purple arrowhead) compared to the adjacent normal hyperintense IV discs.
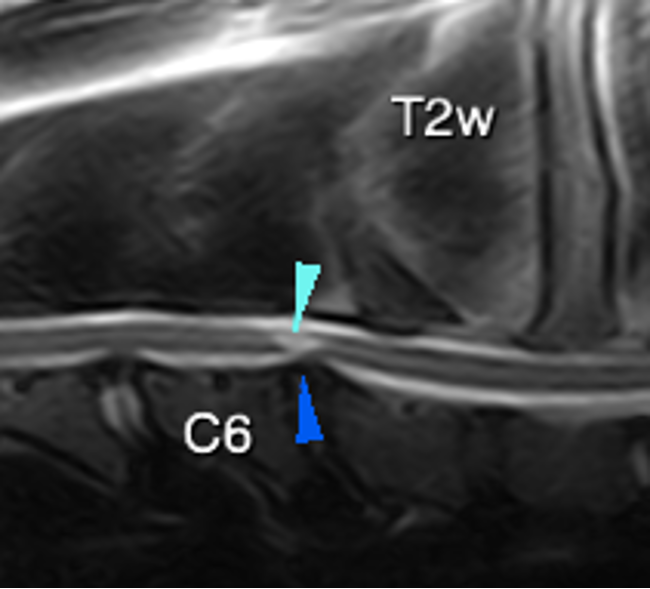
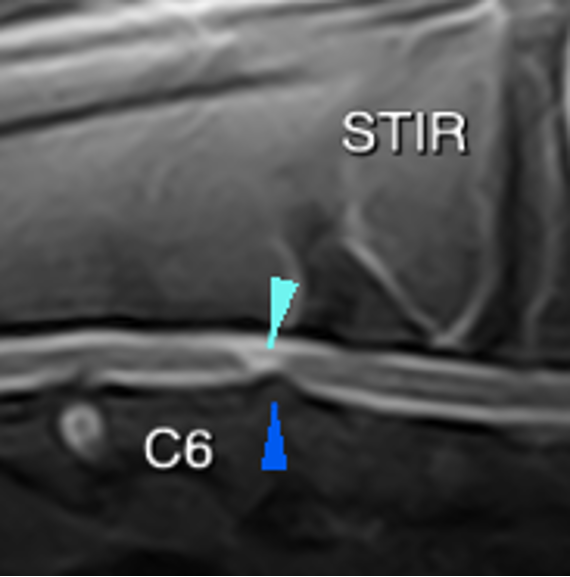
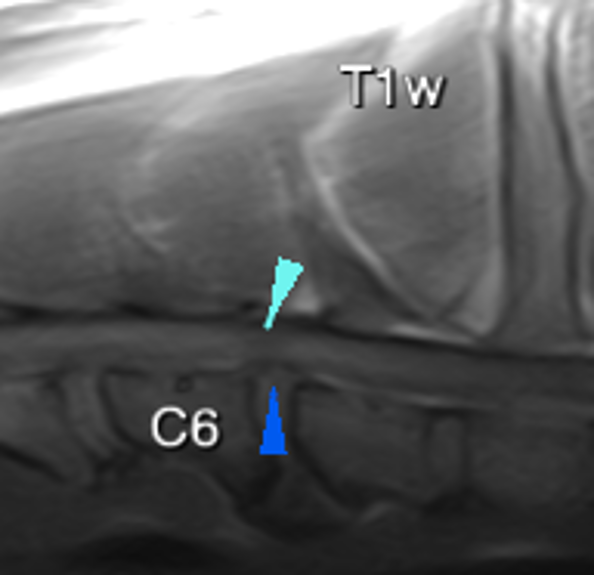
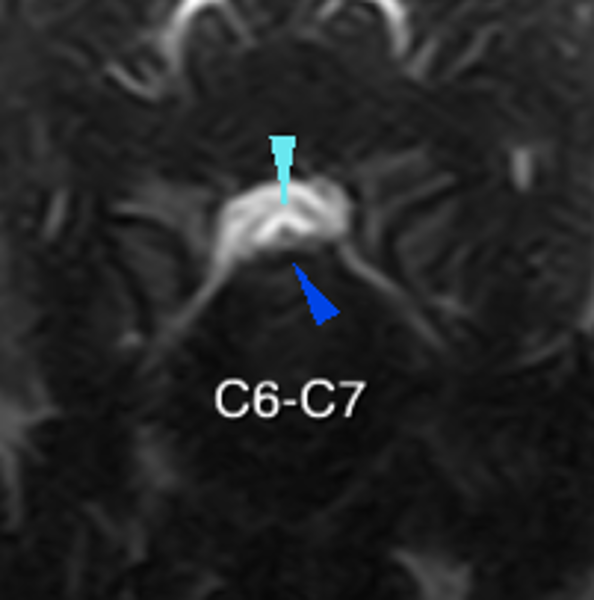
In addition, the IV disc space of C6-C7 is narrower than the rest. The annulus fibrosus of the disc protrudes slightly into the vertebral canal, attenuating the hyperintense ventral signal on T2w but without loss of the dorsal signal (dark blue arrowheads). It causes moderate spinal cord compression. The spinal cord at this level appears to be focally decreased in diameter, with a well-defined intramedullary lesion, hyperintense on T2w and STIR and iso-subtly hypointense on T1w (light blue arrowheads). There is moderate/marked ventral new bone formation (spondylosis).
T2w Sagittal plane
STIR Sagittal plane
T1w Sagittal plane
T2w Transverse plane
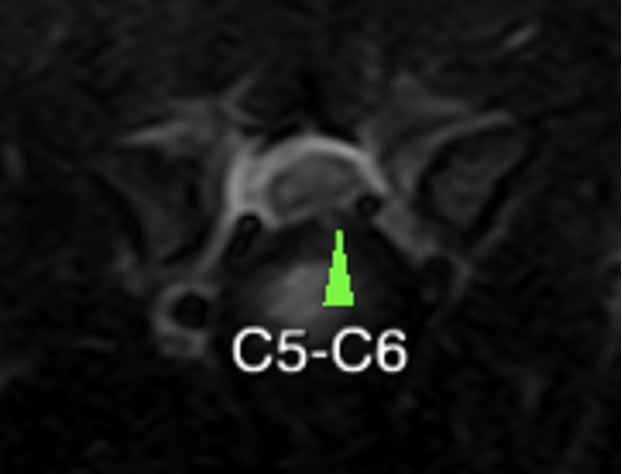
The IV disc of C5-C6 also protrudes subtly into the vertebral canal, centrally and slightly lateralised to the left, causing a very mild compression of the spinal cord (green arrowhead).
Diagnosis
The findings described together are consistent with cervical spondylomyelopathy associated with disc disease:
Changes in the C6-C7 IV space are consistent with intervertebral disc degeneration and protrusion with moderate compressive myelopathy. Secondary focal intramedullary lesion with a slight decrease in spinal diameter, consistent with myelitis/gliosis.
Mild disc protrusion in C5-C6 IV space, slightly lateralized to the left, causing very mild spinal cord compression.
Comments
The findings described together are consistent with cervical spondylomyelopathy associated with disc disease.
Cervical spondylomyelopathy associated with disc disease tends to occur more frequently in the discs that this patient has altered.
The spinal cord compression at C6-C7 is moderate and is associated with an intramedullary lesion with focal decreased diameter of the spinal cord suggesting a chronic and dynamic compression with a greater compression of the cord depending on the positioning of the neck, causing gliosis of the cord. In patients with this condition, a dynamic MRI in neutral position, extension and flexion of the neck may be recommended to observe how compression varies depending on positioning.
(Mon. to Fri. 9 a.m. to 6 p.m. gmt+1) Welcome, How can we help you?
We use cookies to ensure that we give you the best experience on our website. If you continue to use this site we will assume that you are happy with it.Ok


No comment yet, add your voice below!