8-years-old, Great Dane cross Bull Mastiff. Presented with flaccid tail, pain in the right groin and haematochezia. A CT-scan of the thoracolumbar spine and hips was performed.

Description
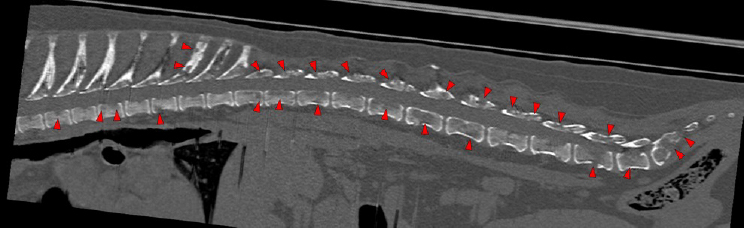
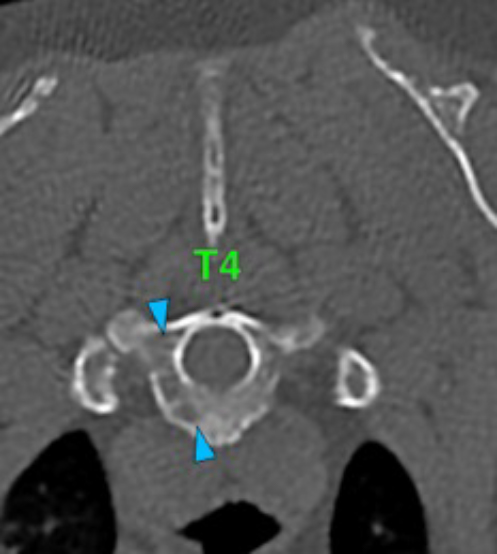
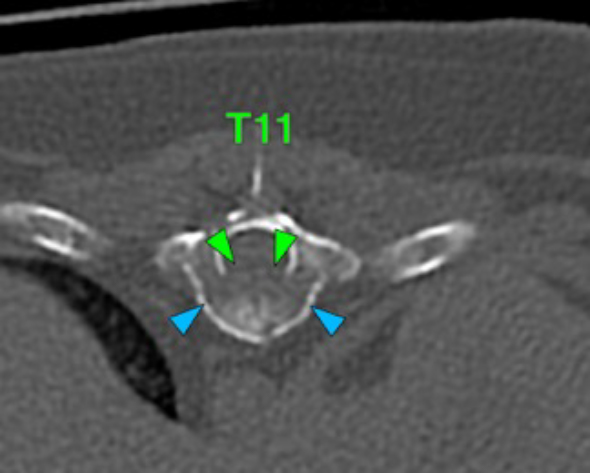
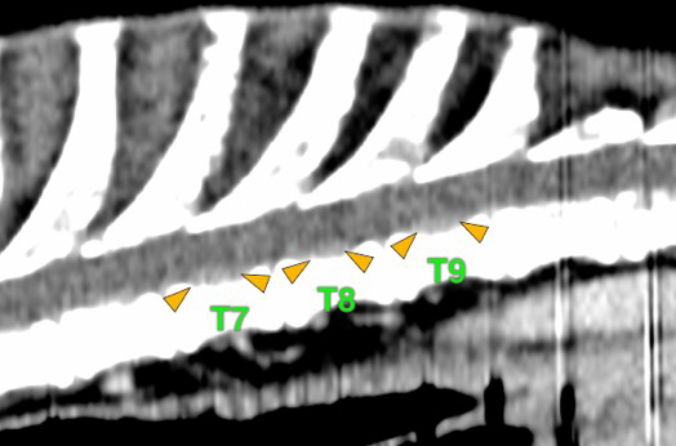
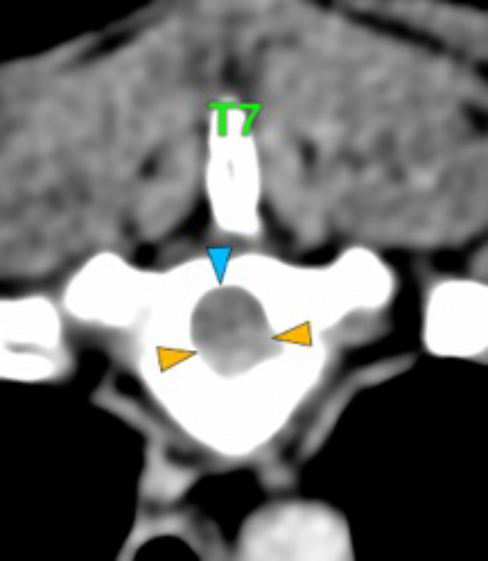
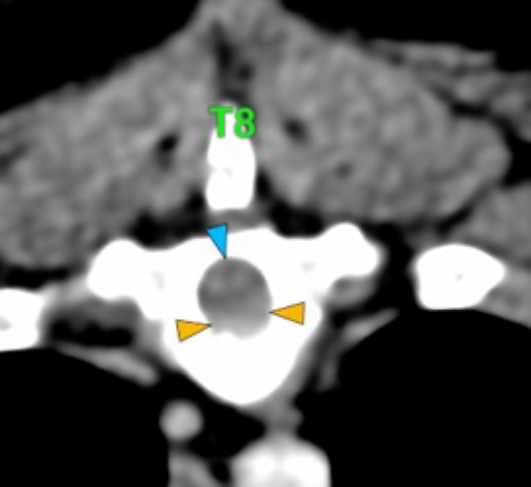
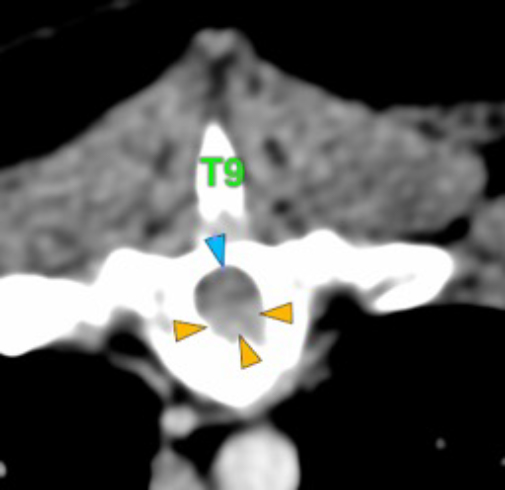
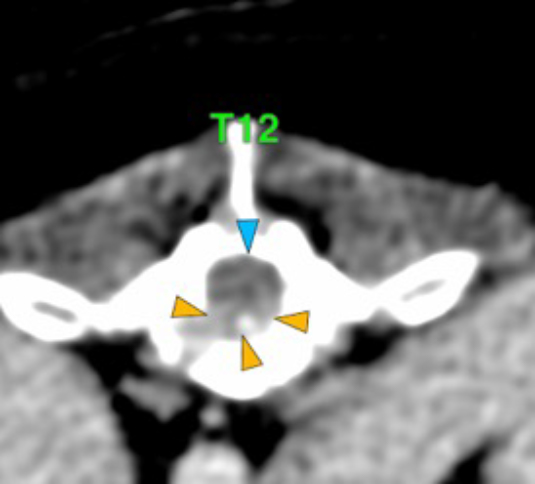
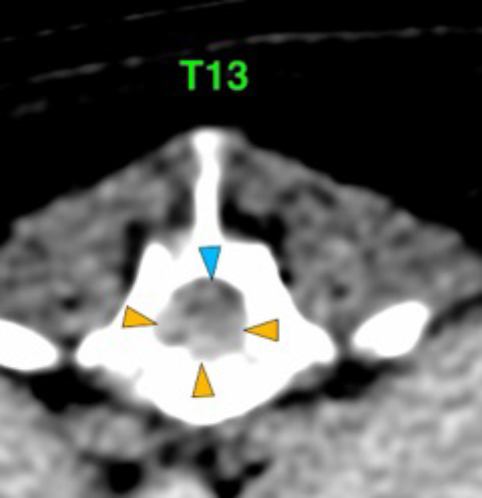
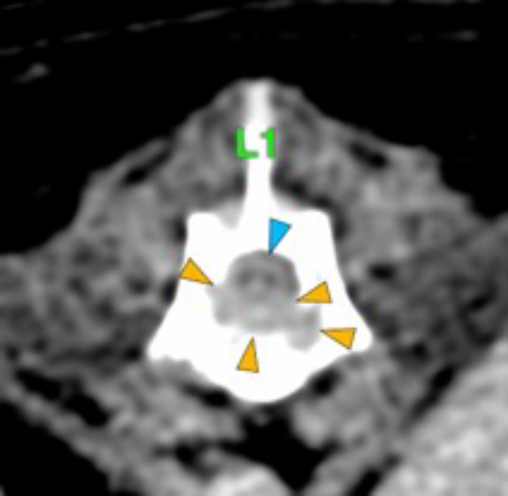
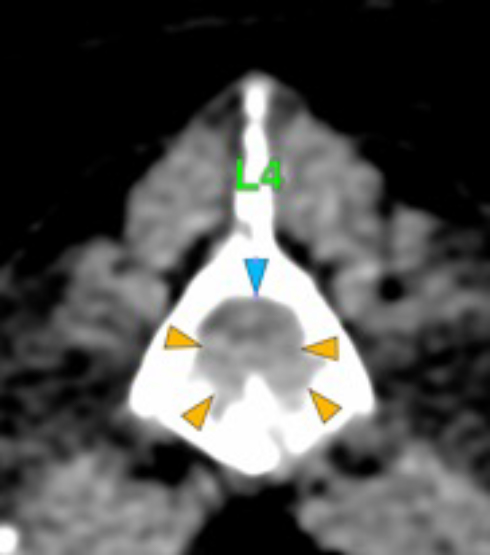
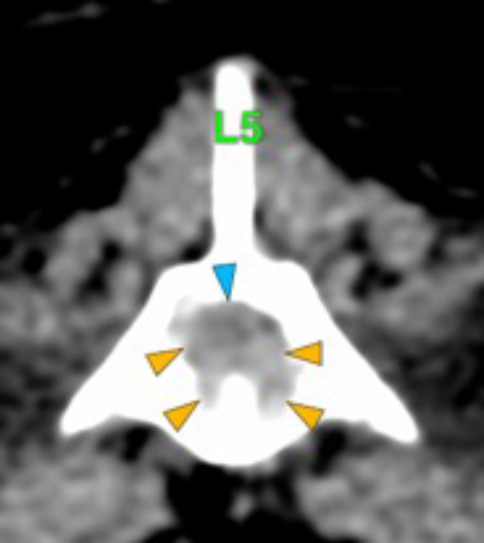
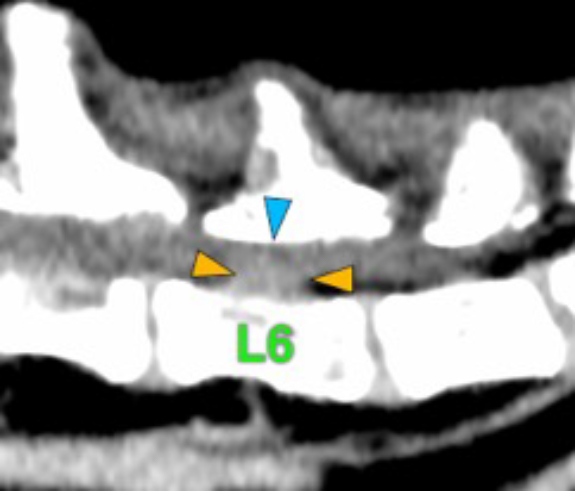
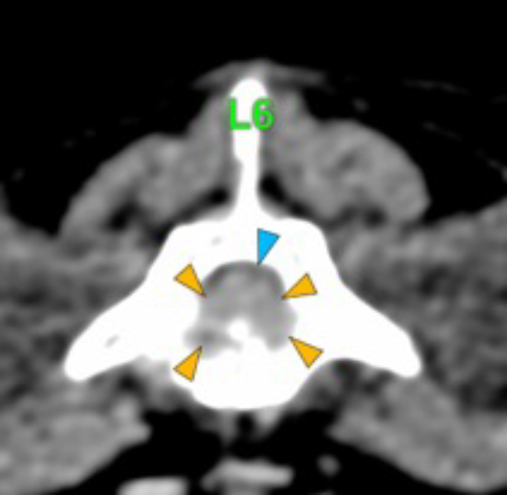
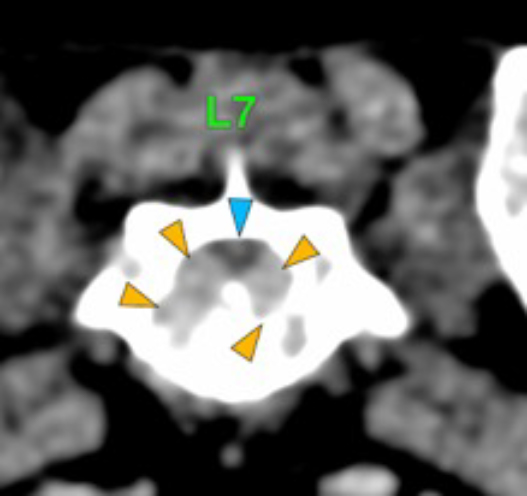
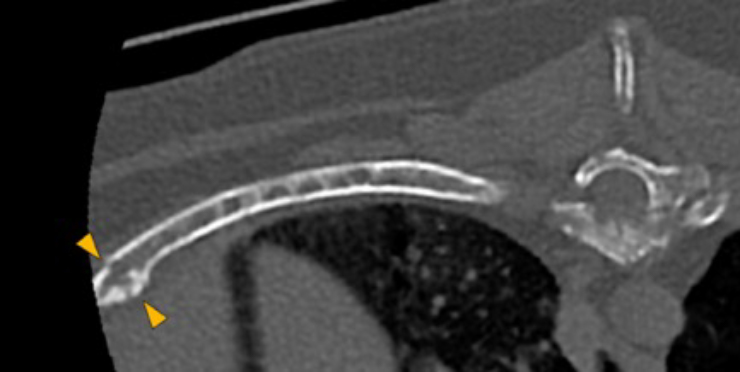
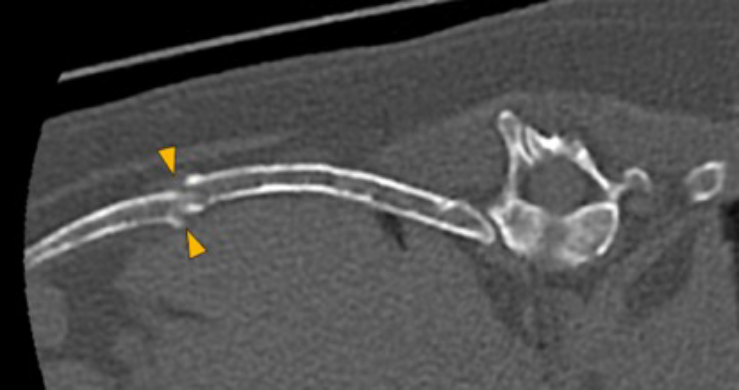
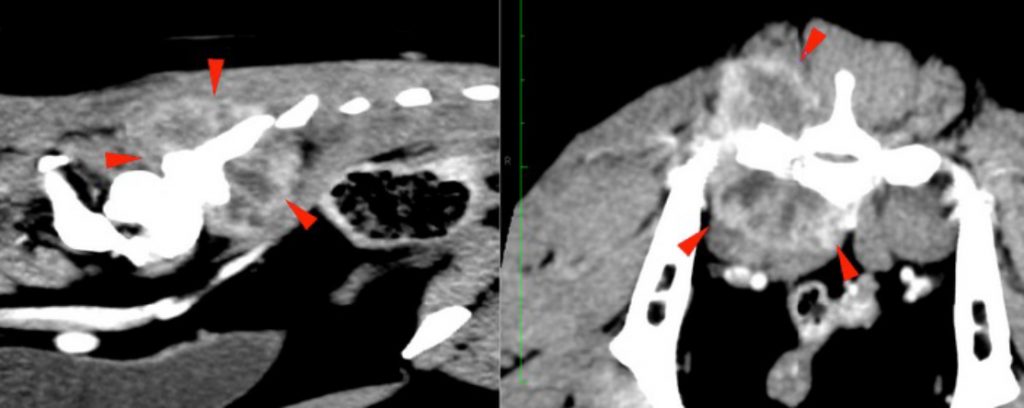
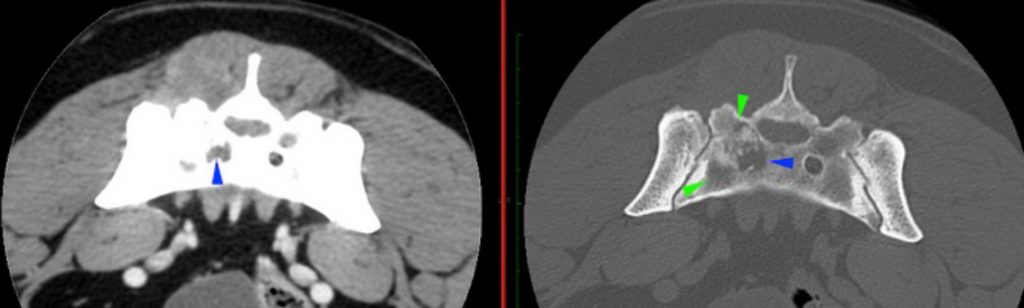
There is a well-defined, irregular to ovoid mass centred at the right caudal aspect of the sacrum (red arrowheads). It is soft tissue attenuating with mineral attenuating foci medially and showing heterogeneous strong contrast enhancement with hypoattenuating and poorly enhancing areas within. It is causing the moth-eaten lysis of the right body of the sacrum (green arrowheads) with irregular margination of the right ventral sacral foramina (blue arrowheads). There is a periosteal reaction noted dorsal to the right sacroiliac joint and ventral caudal sacral body. The mass is invading the sacral canal to this level with complete attenuation of the perineural fat at the level of the right ventral sacral foramina.
The right medial iliac lymph nodes are prominent compared to the left, preserving normal shape and measuring 9 mm in width. They show normal attenuation and contrast enhancement.
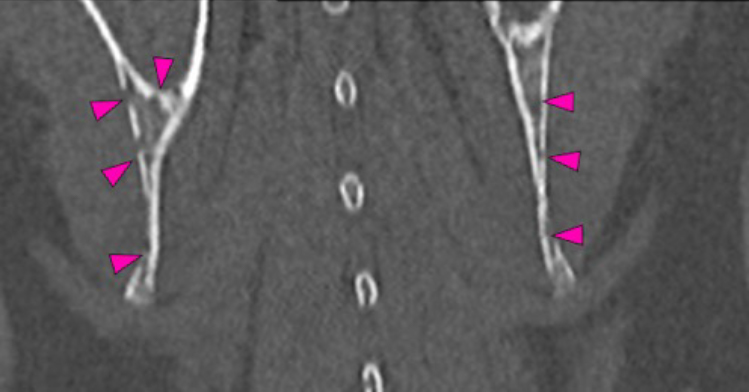
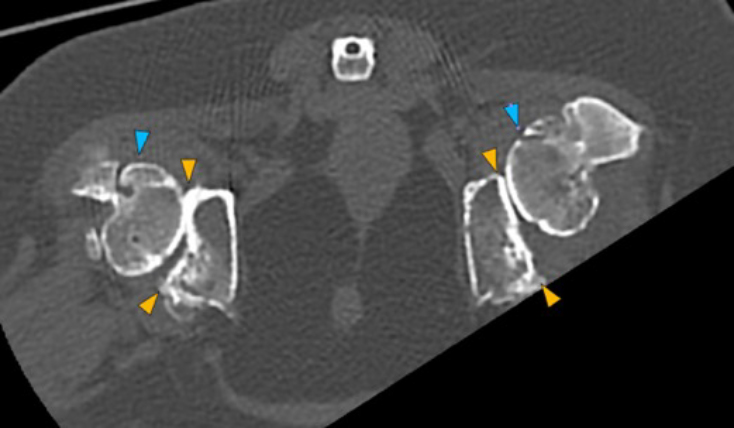
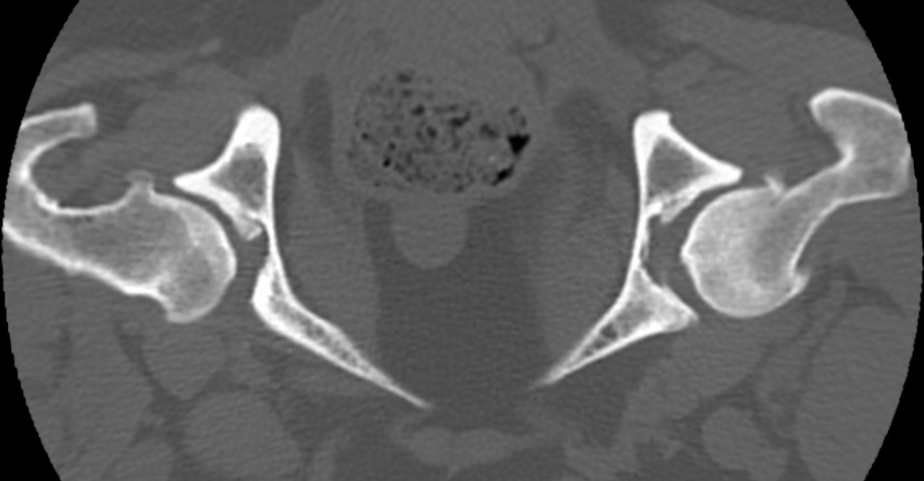
There is bilateral mild periarticular new bone formation at the femoral heads and necks and cranial and caudal acetabular margins (see image below). There are mineral attenuating foci noted at the level of the right lesser trochanter.
Diagnosis
- Aggressive mass centred at the right caudal sacrum compatible with malignant neoplasia (soft tissue sarcoma, primary bone tumour such as osteosarcoma, chondrosarcoma, less likely nerve sheath tumour or round cell tumour). Non-neoplastic processes are considered highly unlikely (granuloma, abscess).
- Right medial iliac lymphadenomegaly. Ddx. Reactive lymphadenopathy, neoplastic infiltration.
- Bilateral osteoarthrosis of the coxofemoral joints.