Abscess and multiple fistulas secondary to a foreign body, causing cholecystitis in a dog
Nine-years old male German Shepherd was presented with recurrent inflammation in different areas of the costal wall and ventral abdomen. He had previous history of foreign body removal (palm tree spike). Dense serosanguinous fluid has been drained from this area and it was consistent with septic exudate. A CT of the thorax and abdomen was performed.
Description
A large cavitary lesion with slightly ill-defined margins is observed along the ventral and lateral aspect of the right caudal thoracic and cranial abdominal wall. The lesion presents several cavities/ramifications (fistulas), with a fluid attenuating non-contrast enhancing core surrounded by a capsule with strong peripheral contrast enhancement.
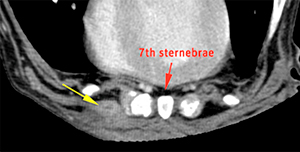
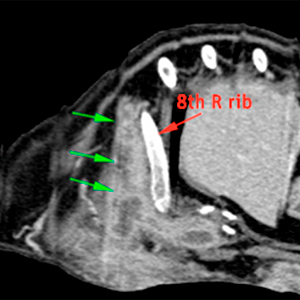
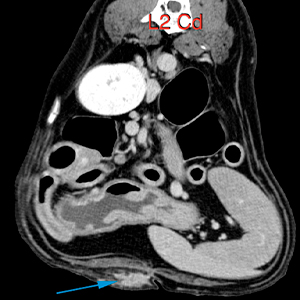
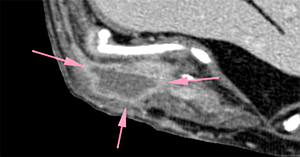
The lesion originates from the ventral costal wall at the cranial aspect of the 7th sternebrae (yellow arrow) extending caudally and laterodorsally along the 7th intercostal space, cranial to the right 8th rib (green arrows) and caudally along the ventrolateral aspect of the abdominal wall. The lesion ends near the linea alba in the mid-abdomen (caudal to L2-L3) (blue arrow), measuring approximately 22 cm in length.
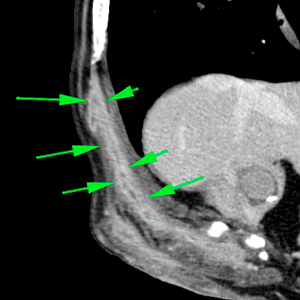
The following images show the path of the previously described lesion, from its origin in the thoracic wall to its end in the abdominal wall.
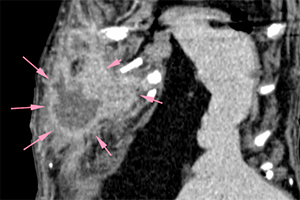
The lesion is largest at the ventral aspect of the 9th and 10th costochondral junctions of the right ribs, where it can be seen as a cavity with ill-defined margins, with a hypoattenuating center (fluid), surrounded by a thick capsule with irregular margins that shows a marked contrast enhancement (pink arrows).
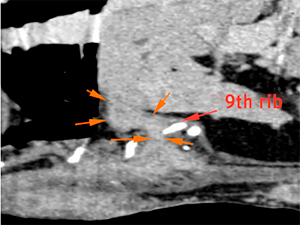
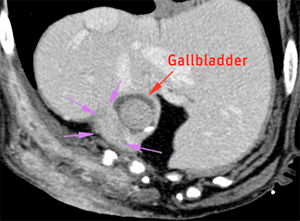
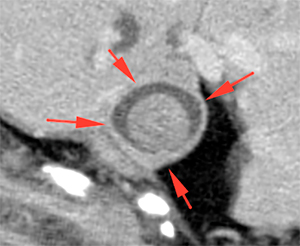
Adjacent to this region, the lesion continues as a markedly contrast-enhancing fistulous tract that extends into the abdominal cavity, ventral to the liver (orange arrows), in contact/attached to the gallbladder (violet arrows). The gallbladder has an abnormal and irregular shape, especially in the area adjacent to the lesion, showing a thickening of its wall (red arrows). The gallbladder is filled with a material increased in attenuation compared to normal bile, with well defined margins and rounded shape.
Diagnosis
Lesion along the right costal/abdominal wall, consistent with an abscess/granuloma secondary to a foreign body. This abscess presents multiple fistulous tracts, one extending dorsolaterally in the 7th intercostal space; and another with intra-abdominal extension. The latter appears to present adhesions and involve the wall of the gallbladder.
Findings at the gallbladder consistent with cholecystitis secondary to adhesions/affection of the gallbladder wall involved in the fistulous tract. A rupture or small laceration of the gallbladder wall cannot be completely ruled; however, there are no signs of biliary peritonitis at the time being.
Comments
The lesion in the costal/abdominal wall is consistent with an abscess/granuloma secondary to a foreign body, considering the imaging findings and patient’s history, even if the foreign body is not visible in the CT. Consider ultrasonographic assessment of the region, including the abdomen, paying special attention to the gallbladder, given that the lesion has intra-abdominal extension. In view of a possible surgical procedure, consider that this lesion may present adhesions/invasion of the adjacent hepatic parenchyma and gallbladder.
(Mon. to Fri. 9 a.m. to 6 p.m. gmt+1) Welcome, How can we help you?
We use cookies to ensure that we give you the best experience on our website. If you continue to use this site we will assume that you are happy with it.Ok


No comment yet, add your voice below!