Cholangiohepatitis with fistulous tract associated with the gallbladder in a dog
2-year-old, female neutered Yorkshire Terrier. She was brought to the vet with apathy, peritoneal effusion, abdominal pain and fever. The analysis of the free fluid in the abdomen is compatible with bile peritonitis. An abdominal CT was performed.
REPORT
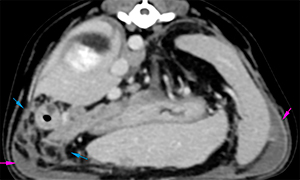
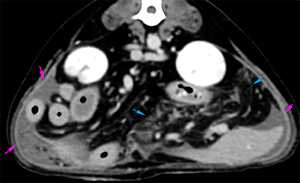
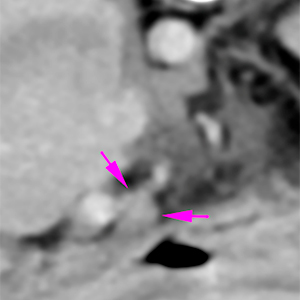
In the abdominal cavity there is a mild/moderate amount of free fluid, with homogeneous attenuation (18 HU) (pink arrows). The vascularization of the peritoneum is prominent, with areas of fat stranding distributed throughout the peritoneum (blue arrows).
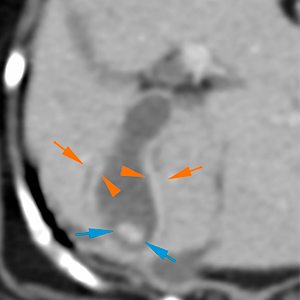
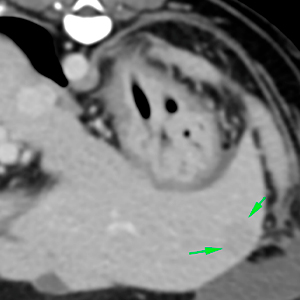
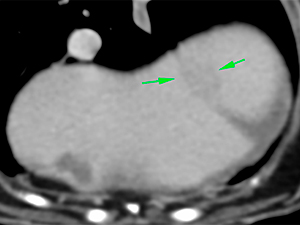
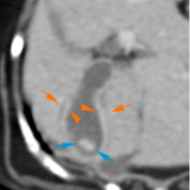
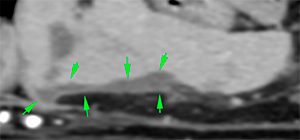
The liver is generally enlarged, with slightly rounded margins (orange arrows), showing a homogeneous attenuation and slightly heterogeneous post-contrast enhancement, with some nodular, hypoattenuating lesions with ill-defined margins (green arrows).
The gallbladder is slightly distended, with a mildly prominent wall presenting a mild hypoattenuating halo (orange arrows). In its depending portion, there is a mineral attenuating structure, with well-defined margins, consistent with a cholelith (blue arrows).
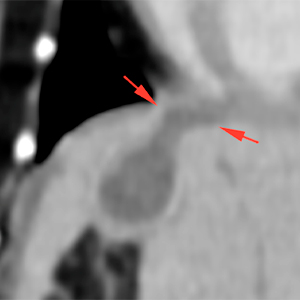
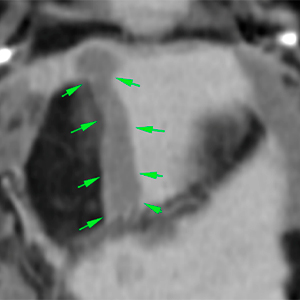
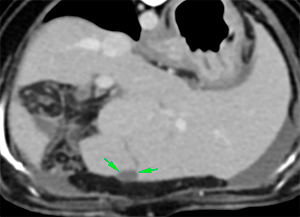
In the cranioventral aspect of the gallbladder, there is a slightly irregular region (red arrows), connected to a tubular tract with well-defined margins that extends caudally along the ventral aspect of the liver, associated to the quadrate liver lobe (green arrows).
One of the hepatic lymph nodes is mildly prominent (5.5 mm in thickness), showing a homogeneous contrast enhancement (pink arrows).
conclusions
Moderate hepatomegaly, with multiple ill-defined hypoattenuating nodules. This is consistent with hepatopathy: inflammatory, vacuolar or neoplastic infiltration, less likely.
Mild thickening of the gallbladder´s wall, with a cholelith, consistent with cholecystitis, with no obvious signs of biliary obstruction.
Possible tubular tract connecting with the gallbladder, consistent with a fistulous tract associated with a possible laceration of the gallbladder’s wall.
Moderate peritoneal effusion and reactive peritoneum, consistent with bile peritonitis, most likely, considering the findings and history of the patient (fluid analysis). Other types of effusion cannot be ruled out based on the CT scan.
Mild hepatic lymphadenopathy, probably reactive.
Comments
The findings are consistent with cholangiohepatitis, most likely, with lesions that may suggest laceration of the gallbladder, with presence of a possible fistulous tract adjacent to the quadrate liver lobe. Considering that the results of the abdominal effusion suggest bile peritonitis, exploratory laparotomy is recommended in this case.
(Mon. to Fri. 9 a.m. to 6 p.m. gmt+1) Welcome, How can we help you?
We use cookies to ensure that we give you the best experience on our website. If you continue to use this site we will assume that you are happy with it.Ok


No comment yet, add your voice below!