Diffuse pneumopathy, pulmonary hypertension and multifocal pulmonary thromboembolism in a dog
9-years-old male Yorkshire Terrier with dyspnea and pulmonary hypertension diagnosed by echocardiography. A thoracic CT-scan was performed.
A thoracolumbar spine and thoracic CT scan was performed.
Description
There is a generalized reduction in volume of all the lung lobes. There is a diffuse, soft tissue attenuation (ground-glass pattern), heterogeneously distributed throughout the lung parenchyma. In many regions, this pattern shows a marked peripheral distribution (orange arrows). There are areas of alveolar pattern in the right cranial and middle lung lobes, and in the left cranial lung lobe (cranial and caudal segments) with a ventral distribution. Many of these areas are associated with a reduction in volume (yellow arrows).
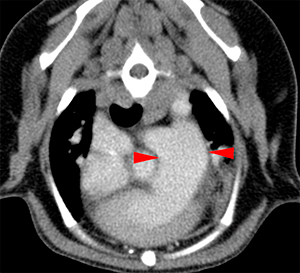
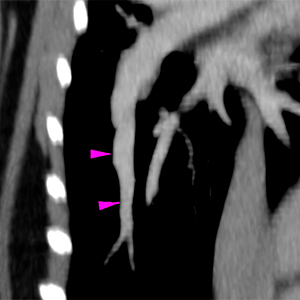
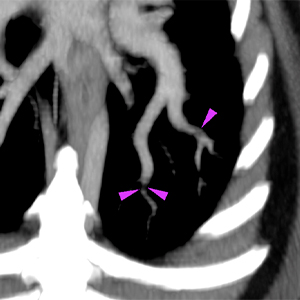
The right ventricle is moderately distended with mild diffuse concentric thickening of its wall. The pulmonary trunk is also markedly dilated (red arrowheads) compared to the descending aorta. The pulmonary arteries are very dilated compared to the veins and with a slightly tortuous path (pink arrowheads). At the distal tributary arteries of the left caudal lobar artery, there are a couple of regions with an abrupt reduction in diameter and focal filling defects on the post-contrast series (violet arrowheads). Similar but less defined changes are seen in the peripheral arterial branches of the right caudal lobe.
On the spine of the right scapula, there is a round, geographical lytic lesion, that does not affect the cortex, with a short transitional zone (well defined) (red arrow). There are a couple of similar lesions affecting the spinous process of T3 and left pedicle of T13 (blue arrows).
Diagnosis
Diffuse pneumopathy, mainly with peripheral and ventral distribution, signs of pulmonary hypertension (dilatation of the pulmonary trunk and arteries) and probable multifocal pulmonary thromboembolism at the level of the arterial branches. Differential diagnosis to consider include: parasitic pneumopathy (e.g. Dirofilariasis, Angiostrongyliasis) with secondary pulmonary thromboembolism, other pneumopathies (e.g. idiopathic pulmonary fibrosis, chronic interstitial pneumonia) with secondary cor pulmonale, thromboembolic pneumonia, or chronic primary pulmonary thromboembolism with secondary pulmonary hypertension and multifocal pulmonary infarcts.
Comments
It is recommended to test for Dirofilaria and Angiostrongylus, perform bronchoalveolar lavage, if clinically indicated, and to rule out systemic diseases that may predispose to thromboembolism (e.g. hyperadrenocorticism, protein-losing nephropathy or enteropathy) in order to reach a definitive diagnosis.
(Mon. to Fri. 9 a.m. to 6 p.m. gmt+1) Welcome, How can we help you?
We use cookies to ensure that we give you the best experience on our website. If you continue to use this site we will assume that you are happy with it.Ok




No comment yet, add your voice below!