2-year-old male Yorkshire Terrier, with a history of neurological symptoms. Pre- and post-prandial bile acids and liver enzymes are elevated. Suspicion of portosystemic shunt. An abdominal CT scan was performed.
Description
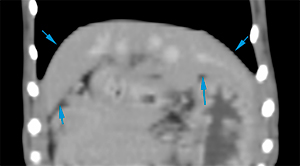
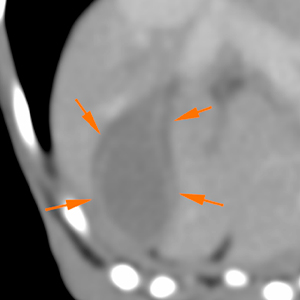
The hepatic parenchyma is reduced in size, causing a cranial displacement of the gastric axis, while preserving smooth and sharp margins, with homogeneous attenuation in the pre- and post contrast studies (during the delayed venous phase) (blue arrows). The gallbladder is filled with a mild amount of hyperattenuating content, and its wall is surrounded by a hypoattenuating halo (orange arrows).
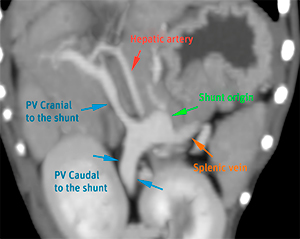
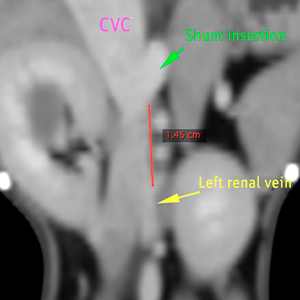
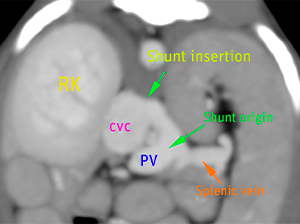
In the portal vein (PV), at the site of insertion of the splenic vein, there is an aberrant vessel (shunt, green arrow) (5.7 mm in diameter), which runs craniodorsally with a very short path, inserting into the left side of the caudal vena cava (CVC), at the level of the cranial pole of the right kidney (insertion – 1.4 cm cranial to the insertion of the left renal vein). The shunt surrounds the hepatic artery.
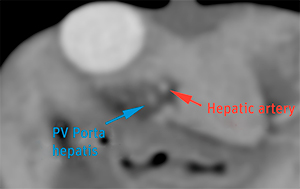
Cranial to the origin of the shunt, the portal vein shows a marked and abrupt reduction in size (from 4.8 mm to 2.5 mm in diameter), extending cranial to the porta hepatis, where it shows a significant reduction in size, similar in size to the hepatic artery. At this level, the portal vein is surrounded by a hypoattenuating halo. The intrahepatic branches of the portal vein are markedly reduced in size and are not clearly visible.
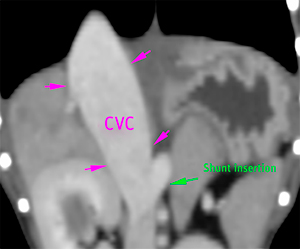
Cranial to the insertion of the shunt, the caudal vena cava is markedly enlarged at its pre- and hepatic portions.
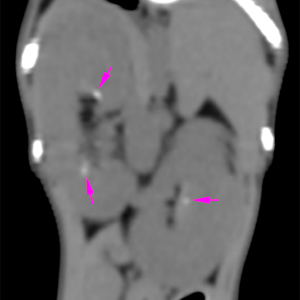
Both kidneys are prominent, while preserving a normal shape. Both have small mineral foci located in the pelvis and renal diverticula (pink arrows).
Diagnosis
Aberrant vessel consistent with congenital extrahepatic portosystemic shunt, most likely. Taking into account its anatomy, this is consistent with a portocaval shunt (splenocaval), inserting on the left side of the caudal vena cava at level of the cranial pole of the right kidney.
Marked reduction in size of the portal vein, cranial to the origin of the shunt, surrounded by a hypoattenuating halo, which could indicate some degree of portal hypertensio
Hypoattenuating halo surrounding the gallbladder, consistent with oedema of the wall secondary to portal hypertension or inflammatory changes.
Microhepatia and mild bilateral renomegaly, secondary to the shunt.
Comments
Evaluation of the portal flow is recommended in order to determine whether portal hypertension is present.
(Mon. to Fri. 9 a.m. to 6 p.m. gmt+1) Welcome, How can we help you?
We use cookies to ensure that we give you the best experience on our website. If you continue to use this site we will assume that you are happy with it.Ok


No comment yet, add your voice below!