Six-year-old male DSH with a 1-month history of tachypnea. A thoracic and abdominal CT was performed.
Description
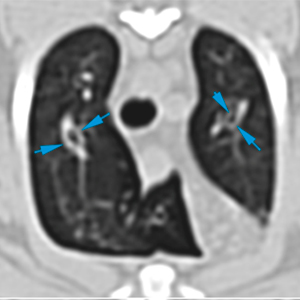
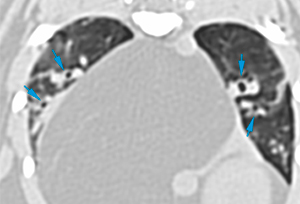
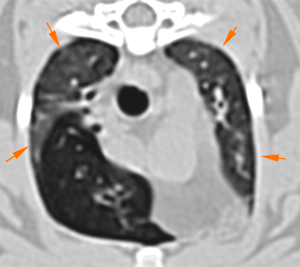
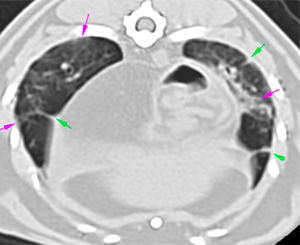
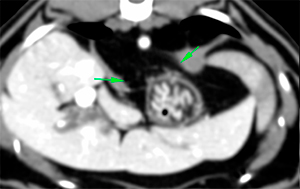
There is a mild diffuse bronchial wall thickening affecting all the lung lobes (blue arrows), with mild diffuse increased attenuation of multiple lung lobes (ground-glass attenuation) (orange arrows) and patchy areas at the caudal lung lobes (pink arrows): There are also multiple parenchymal bands (green arrows).
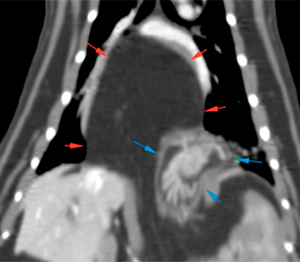
There is a wide defect (approx. 2.3 cm) (green arrows) in the dorsal and central aspect of the diaphragm. Through this defect, a marked amount of mesenteric fat (red arrows) and part of the gastric fundus (blue arrows) extends into the thoracic cavity.
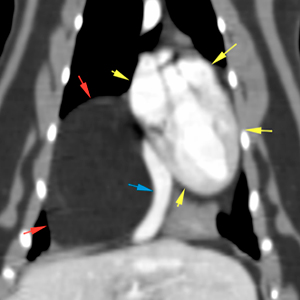
The mesenteric fat causes a displacement of the heart (yellow arrows) and caudal vena cava (blue arrow) to the left and ventrally, with a mild retraction of the right caudal and accessory lung lobes.
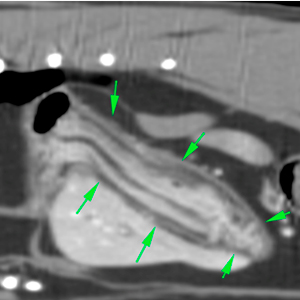
The rest of the gastric fundus, body and pyloric antrum have a normal position in the abdomen (green arrows). No gastric distension is observed.
Diagnosis
Diffuse bronchial wall thickening with areas of diffuse and patchy areas of interstitial attenuation (feline asthma most likely). A pneumonic process cannot be ruled out, although it is less likely.
Diaphragmatic hernia with concurrent herniation of the mesenteric fat and part of the gastric fundus. This causes a slight retraction of the lung lobes, mediastinal deviation, and displacement of caudal vena cava.
Comments
Bronchoalveolar lavage is recommended for further investigation, in relation to the findings in the pulmonary parenchyma. The origin of the hernia is uncertain and may be congenital, most likely, or secondary to trauma, less likely, considering that there are no signs of associated trauma.
(Mon. to Fri. 9 a.m. to 6 p.m. gmt+1) Welcome, How can we help you?
We use cookies to ensure that we give you the best experience on our website. If you continue to use this site we will assume that you are happy with it.Ok


No comment yet, add your voice below!