Feline lung patchy alveolar pattern with fibrosing pleuritis, bilateral pleural effusion and pneumothorax
7-years-old, male, DSH cat with pleural effusion of unknown origin. Lung alveolar pattern was seen on the X-rays. A thoracic CT-scan was performed.
A thoracolumbar spine and thoracic CT scan was performed.
Description
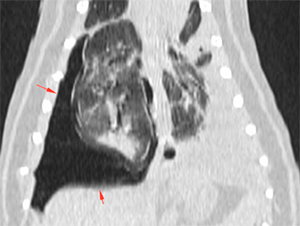
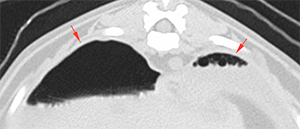
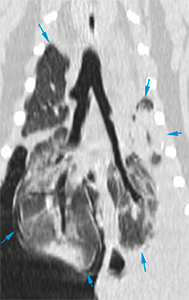
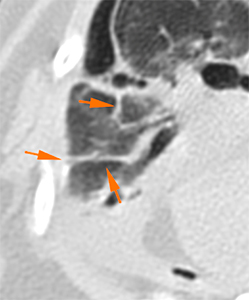
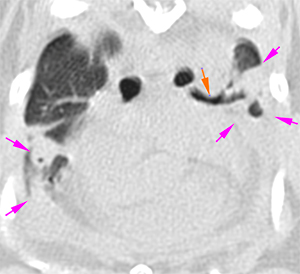
There is a mild/moderate amount of gas in the dorsal pleural space bilaterally, more evident in the right hemithorax (red arrows).
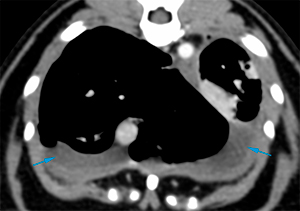
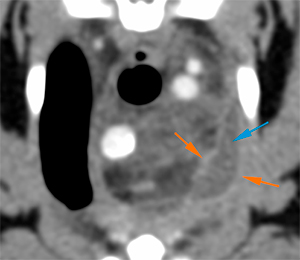
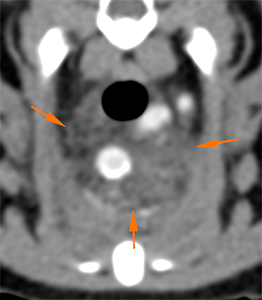
There is a moderate amount of fluid attenuating content (20 HU) in the pleural space bilaterally, located ventrally (blue arrows). The parietal pleura is diffusely thickened in the post-contrast series (orange arrows).
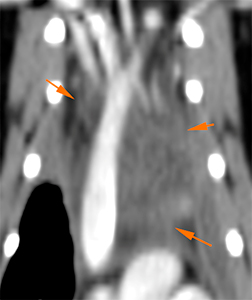
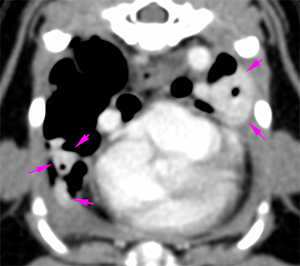
The cranial mediastinum is enlarged with increased and heterogeneous attenuation, showing a striated appearance. There is loss of the normal mediastinal fat attenuation (orange arrows). There are no signs of mass effect on the mediastinal structures.
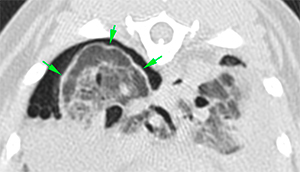
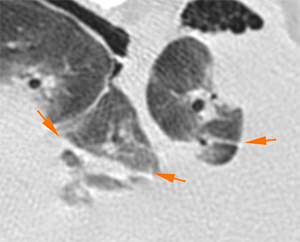
All lung lobes show rounded margins and a variable degree of collapse with loss of volume, being more marked in the left hemithorax (blue arrows) – associated with a greater amount of pleural effusion -. There is also thickening of the visceral pleura of some of the lung lobes showing an irregular surface, being more evident at the right caudal lobe, as it is surrounded by air (green arrows). Multiple subpleural and parenchymal bands are seen in multiple lung lobes (orange arrows).
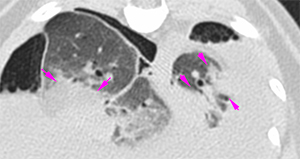
In all lung lobes there are peribronchial areas with patchy increased attenuation (pink arrows), showing a marked extension, with well-defined and slightly irregular margins, generating the presence of air bronchograms (orange arrow). These areas show a marked and homogeneous contrast enhancement. In some of them, there are small mineral attenuating foci in the periphery. The left and right caudal lung lobes are the most affected ones.
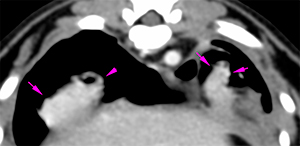
The diameter of the lobar bronchi of the right cranial lung lobe is widened along its entire path up to its most peripheral portion, with cylindrical morphology – bronchiectasis – (red arrows).
Diagnosis
Diffuse areas of extensive peribronchial infiltrates with coalescence in an alveolar pattern, most likely consistent with a chronic inflammatory/infectious process (pneumonic process: interstitial pneumonia, bacterial, etc.). Other differential diagnosis such as pulmonary fibrosis or neoplastic process, cannot be ruled out.
Moderate bilateral pleural effusion and diffuse thickening of the parietal and visceral pleura, most likely consistent with fibrinous pleuritis associated to chronic effusion.
Mild bilateral pneumothorax consistent with iatrogenic after chest drainage or ex vacuo pneumothorax. Other causes of pneumothorax cannot be ruled out.
Thickening and increased attenuation of the mediastinum, consistent with oedema +/- inflammation of the cranial mediastinum (mediastinitis), probably reactive to the chronic pulmonary process and the presence of effusion.
Comments
Bronchoalveolar lavage with sampling and culture and/or FNAs of one of the areas of alveolar infiltrates are recommended in order to reach a definitive diagnosis.
(Mon. to Fri. 9 a.m. to 6 p.m. gmt+1) Welcome, How can we help you?
We use cookies to ensure that we give you the best experience on our website. If you continue to use this site we will assume that you are happy with it.Ok




No comment yet, add your voice below!