10-year-old female French Bulldog. History of tachypnoea and anorexia. Thoracic X-ray showed displacement of the trachea towards the right and loss of visualisation of the cranial margins of the cardiac silhouette with increased opacity of the cranial lung lobes.
Description
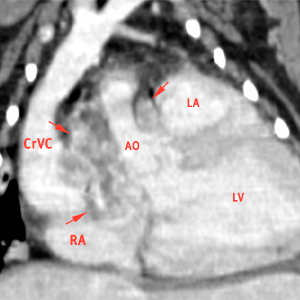
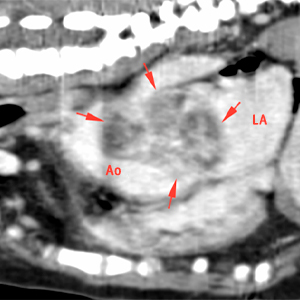
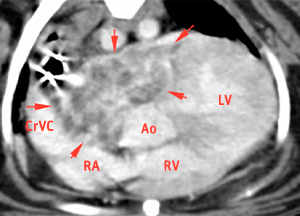
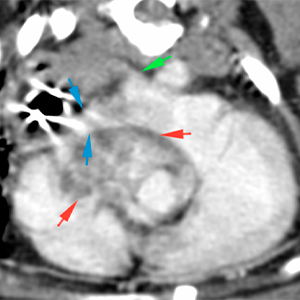
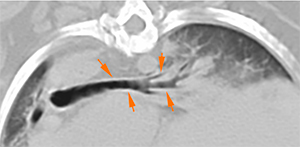
There is a soft tissue attenuating mass with irregular margins, showing heterogeneous contrast enhancement, at the level of the cardiac base (red arrows). This mass is visualised on the right side of the base of the aorta extending cranially around the aortic arch. The mass causes a rightward displacement of the cranial vena cava (CrVC) and right atrium (RA), as well as a caudal displacement of the left atrium (LA), although there is no clear invasion of these structures by the mass.
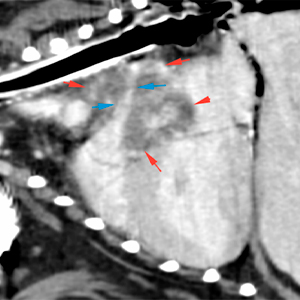
The right pulmonary artery (blue arrows) is surrounded by the mass and slightly compressed, but with no obvious filling defects. The left pulmonary artery is unremarkable (green arrow).
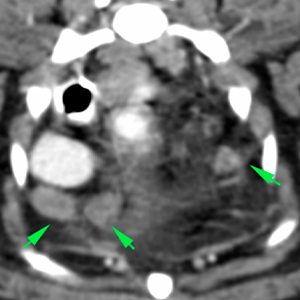
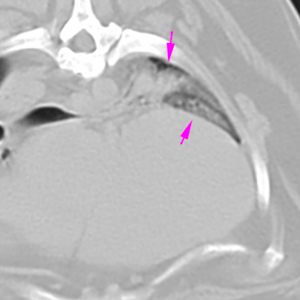
There is a moderate enlargement of cranial mediastinal and tracheobronchial lymph nodes, showing homogeneous post-contrast enhancement (green and orange arrows respectively).
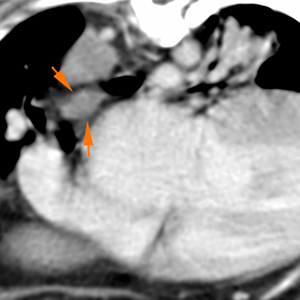
The trachea is markedly displaced towards the right in the cranial mediastinum and at the level of the carina (orange arrows), which is partly due to a mild mass effect caused by the mass previously described, and partly due to an anatomical variation related to the patient’s breed.
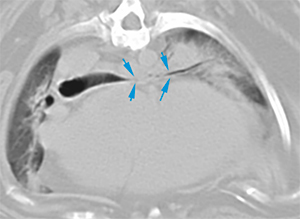
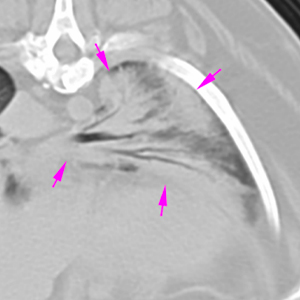
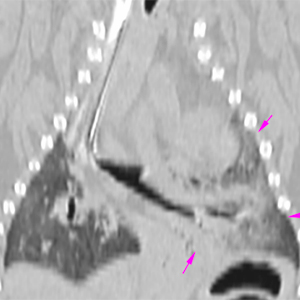
The heart is slightly prominent, occupying a large portion of the left cranial hemithorax. This causes a marked narrowing of the lobar bronchus of the left cranial lung lobe, affecting both cranial and caudal segments (blue arrows) and mild narrowing of the lobar bronchus of the left caudal lung lobe (orange arrows). These lung lobes are diffusely increased in attenuation, with presence of air bronchograms and a reduced volume (pink arrows), showing a homogeneous post-contrast enhancement.
Diagnosis
Heart base mass, associated with the aortic arch, consistent with a neoplastic process (chemodectoma, more likely vs. others such as haemangiosarcoma, etc. less likely).
The mass causes a mild/moderate mass effect on the main vessels and cardiac chambers, without obvious invasion.
Moderate cranial mediastinal and tracheobronchial lymphadenopathy, consistent with metastasis vs. reactive.
Possible cardiomegaly.
Tracheal displacement towards the right, mild/moderate collapse and displacement of the left lobar bronchi, more severe in the cranial lung lobe, caused by the mass in conjunction with possible cardiomegaly.
The changes in the lung parenchyma changes are most likely consistent with atelectasis. Other differentials such as a pneumonic process are less likely, although cannot be excluded.
Comments
Echocardiographic evaluation is recommended to assess cardiac functionality. The changes in the pulmonary parenchyma seem to be consistent with atelectasis, possibly secondary to the conformation of the patient’s thoracic cavity, together with possible cardiomegaly and mass effect caused by the mass at the level of the cardiac base. Histopathological analysis of the cardiac mass is required to reach a definitive diagnosis.
(Mon. to Fri. 9 a.m. to 6 p.m. gmt+1) Welcome, How can we help you?
We use cookies to ensure that we give you the best experience on our website. If you continue to use this site we will assume that you are happy with it.Ok



No comment yet, add your voice below!