2 year-old male Weimaraner. He is referred with a history of recurrent hypersalivation, anorexia and weight loss, with a favourable response to treatment (antibiotics and glucocorticoids). The symptoms always recur after cessation of treatment. Possible oropharyngeal foreign body.
Along with the CT scan, an oropharyngeal examination was performed, observing glossitis and laryngitis, with an ulcerative and purulent appearance.
A thoracic and head CT scan was performed
Description
Head
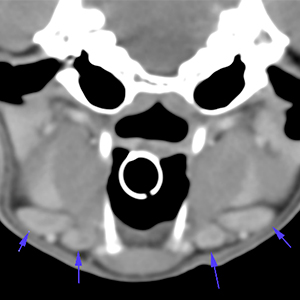
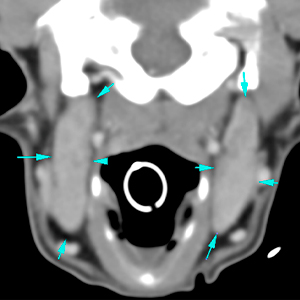
The mandibular (dark blue arrows), and the medial retropharyngeal lymph nodes (light blue arrows), are mildly/moderately enlarged, with smooth margins and homogeneous parenchyma.
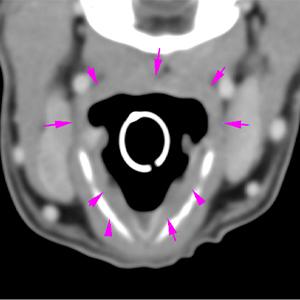
The pharyngeal/laryngeal mucosa appears mildly and diffusely thickened (purple arrows), with no association to mass or nodular lesions. There are no cavitary or mass-like lesions, or foreign bodies in the retropharyngeal / cervical region.
Thorax
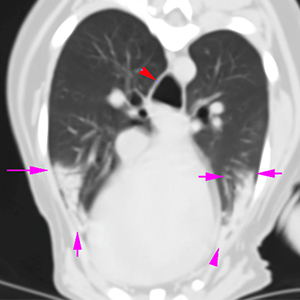
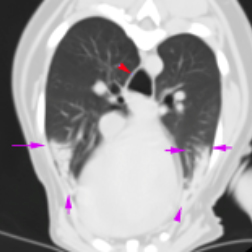
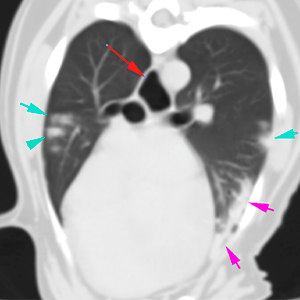
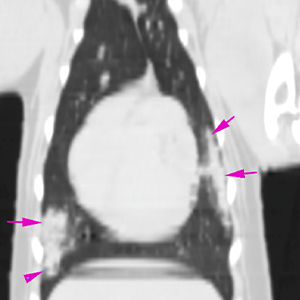
The pulmonary parenchyma is predominantly aerated and expanded, although there are several dependent areas affecting the ventral regions of the right middle and the caudal segment of the left cranial lung lobes, showing a loss of aeration and increased soft tissue attenuation with presence of air bronchograms, while the lung volume is mostly preserved (purple arrows). At this level, there are several small subpleural foci adjacent to the regions previously described, affecting also the right cranial lung lobe (blue arrows).
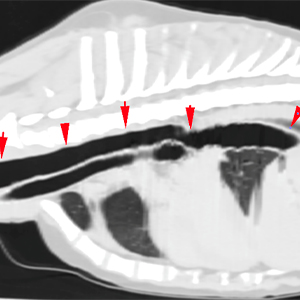
The oesophagus is mildly/moderately distended with gas in its cervical and thoracic portions (red arrows), with presence of a slight amount of intraluminal fluid in the caudal oesophagus.
Diagnosis
Bilateral mild/moderate lymphadenomegaly of the mandibular and medial retropharyngeal lymph nodes. Reactive lymphadenopathy (inflammatory, infectious) most likely; an infiltrative neoplastic process is considered unlikely.
Possible laryngitis / pharyngitis. This is a subtle and non-specific finding, that could be due to an inflammatory, immune-mediated or infectious process (bacterial, viral, etc.)
There are focal areas of alveolar pattern, with a predominantly apical ventral and subpleural distribution, affecting the right middle, left cranial and, to a lesser extent, right cranial lung lobes. These changes are suggestive of pulmonary consolidation (e.g. aspiration pneumonia, inflammatory infiltrates, infectious bronchopneumonia). Atelectasis cannot be ruled out, although a greater reduction in volume would be expected, and worst delimitation in comparison to the aerated parenchyma.
The mild / moderate generalized oesophageal distention could be secondary to the anaesthesia, esophagitis or megaoesophagus (immune-mediated, neuromuscular, idiopathic, metabolic disease). This finding should be evaluated in correlation with the clinical signs.
comments
The changes described suggestive of laryngitis / pharyngitis, associated with regional lymphadenopathy, are non-specific, and could be an inflammatory / immune-mediated or infectious process. There are no lesions suggestive of foreign bodies or abscesses in this region.
In young Weimaraner, a multisystemic inflammatory syndrome associated with a wide range of clinical signs (fever, anorexia, lethargy, gastrointestinal disorders, lameness) has been described. This syndrome can be suspected if the animal presents recurrent signs of inflammatory disease affecting the joints, bones, central nervous system, gastrointestinal tract, skin, urinary tract, or lymph nodes, and / or development of clinical signs after administration of vaccines.
Repeating chest radiographs can help with the evaluation of the changes described and help rule out atelectasis. Consider thoracic ultrasound to assess pulmonary changes and FNAs.
(Mon. to Fri. 9 a.m. to 6 p.m. gmt+1) Welcome, How can we help you?
We use cookies to ensure that we give you the best experience on our website. If you continue to use this site we will assume that you are happy with it.Ok


No comment yet, add your voice below!