Intracranial extension of an expansile ear lesion in a cat
9-year-old, female, Maine Coon was presented with recurrence of a peripheral vestibular syndrome.
A ventral osteotomy of the left tympanic bulla was previously performed. An MRI of the head was performed.
Description
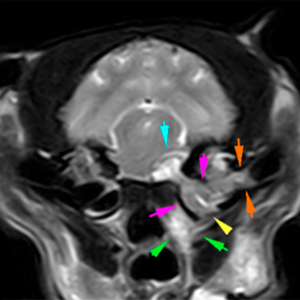
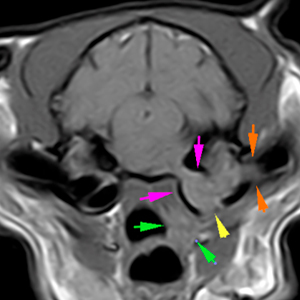
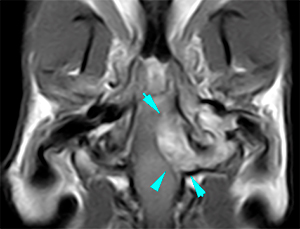
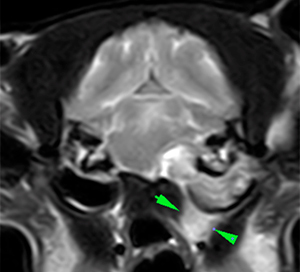
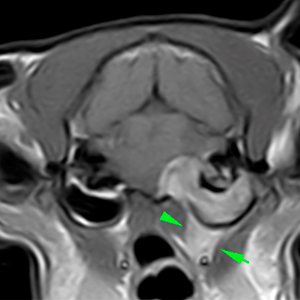
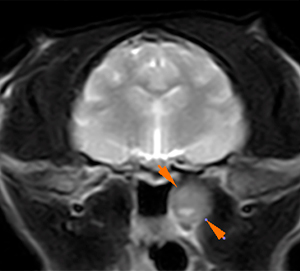
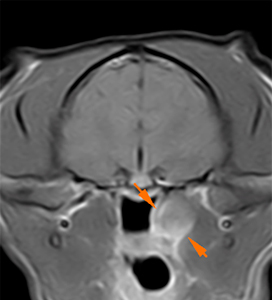
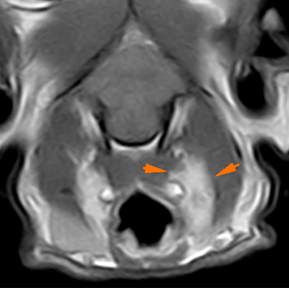
There is a lesion extending from the horizontal portion of the left external ear canal, adjacent to the tympanic membrane (orange arrows), occupying the tympanic bulla (pink arrows) with intracranial extension, as an extra-axial lesion (blue arrows). The lesion shows a mixed signal intensity on T2W, mainly hyperintense compared to the musculature, is slightly hyperintense on T1W and has a marked and homogeneous post-contrast enhancement. The lesion also affects the soft tissues adjacent to the tympanic bulla (green arrows).
Associated with this lesion, there is a mild expansion of the tympanic bulla, with thickening of its wall (pink arrows). In addition, there is a defect in the ventral aspect of the wall of the bulla, corresponding to the location of the previous osteotomy described in the history (yellow arrow).
T2W
T1W
T1W+Gd
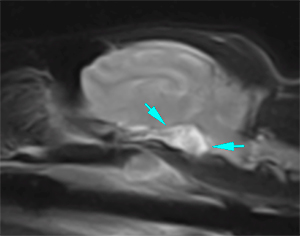
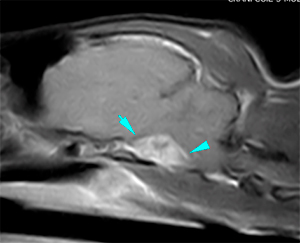
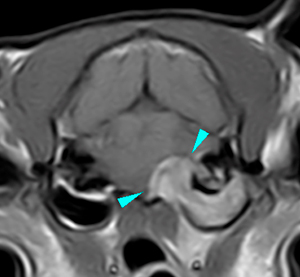
From the tympanic bulla, the lesion extends intracranially through the region of the left petro-occipital canal, invading the region ventral and to the left of the brainstem at the level of the mesencephalon. The lesion has a broad base, with well-defined margins, with the same signal intensity characteristics as those described above, showing a marked and mainly homogeneous post-contrast enhancement, although with some slightly hypointense areas (blue arrows).
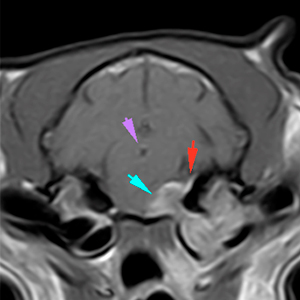
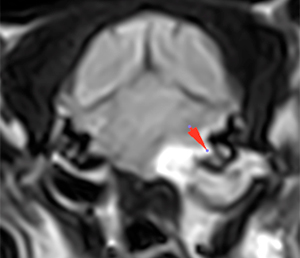
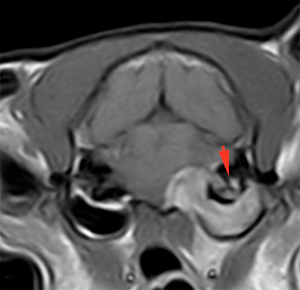
Associated with this mass, there is a marked thickening of the meninges, with presence of a “dural tail” sign (red arrows), and a moderate mass effect over the mesencephalon, with a subtle displacement of the mesencephalic aqueduct to the right (violet arrows).
T2W sagittal plane
T1W+Gd sagittal plane
T1W+Gd dorsal plane
T1W+Gd transverse planes
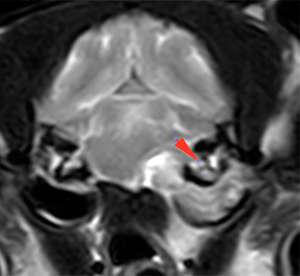
The left inner ear is also affected, showing a mild decreased of the normal hyperintense signal intensity on T2W of the intra-labyrinthic fluid, without suppression in FLAIR and with moderate post-contrast enhancement (red arrows).
T2W
FLAIR
T1W+Gd
Ventral to the left tympanic bulla, there is a lesion that connects with the previously described lesions. This lesion shows ill-defined margins, is hyperintense on T2W, with homogeneous post-contrast enhancement (green arrows) and extends through the region of the left internal ear canal (Eustachian tube) protruding into the left nasopharyngeal wall (orange arrows), without invading it (orange arrows).
T2W
T1W+Gd
T1W+Gd
The left medial retropharyngeal lymph node is slightly more prominent and asymmetric compared to the contralateral side (orange arrows).
T1W+Gd
Diagnosis
Lesion at the level of the left external ear canal and tympanic bulla with intracranial extension (causing an extra-axial lesion) and extending along the internal ear canal and soft tissues ventral to the bulla. These findings are most likely consistent with a neoplastic process (neoplasia originating in the ear with extension to other locations – infiltrative ceruminous gland adenocarcinoma, squamous cell carcinoma, lymphoma, etc. vs originating from the retropharyngeal region and extending to the other locations – paraganglioma less likely). Other differentials, such as an infectious process, are considered unlikely in this case, given the characteristics of the lesions that seem to correspond to a solid mass.
Findings in the left inner ear consistent with invasion of the inner ear by the previously described lesion vs associated otitis interna.
Ipsilateral medial retropharyngeal lymphadenopathy, metastasis most likely vs reactive.
Comments
Sampling of the mass (at the level of left retropharyngeal region or through the external ear canal) is required to reach a definitive diagnosis.
(Mon. to Fri. 9 a.m. to 6 p.m. gmt+1) Welcome, How can we help you?
We use cookies to ensure that we give you the best experience on our website. If you continue to use this site we will assume that you are happy with it.Ok



No comment yet, add your voice below!