Pancreatic mass, with invasion of the gastroduodenal vein and pulmonary metastasis
11-years-old, female, crossbreed dog with hypoglycemia since she was 9 years old. Seizures in the last 24 hours.
A thoracic and abdominal angiography CT-scan was performed.
A thoracolumbar spine and thoracic CT scan was performed.
Description
Abdomen:
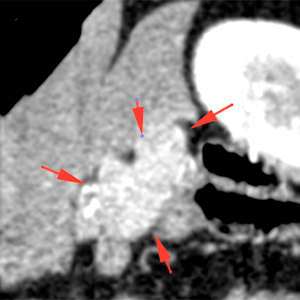
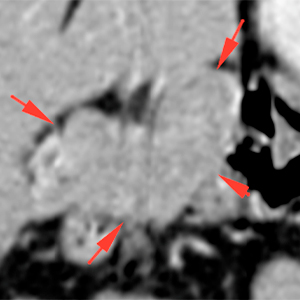
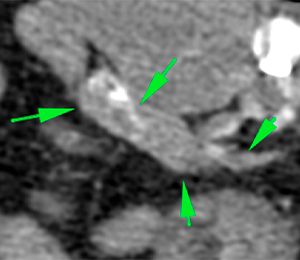
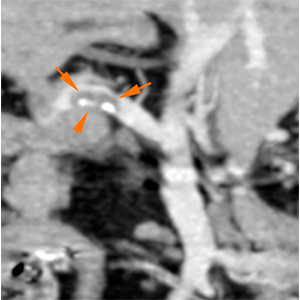
There is a bilobulated, well-defined soft-tissue mass in the caudomedial aspect of the right pancreatic lobe (red arrows). This lesion is heterogeneous, showing a marked and heterogeneous contrast enhancement in the arterial phase; in the early and delayed venous phase this lesion has the same attenuation as the rest of the pancreatic parenchyma. The body and left lobe of the pancreas do not show abnormalities (green arrows).
Pre-contrast
Arterial phase
Venous phase
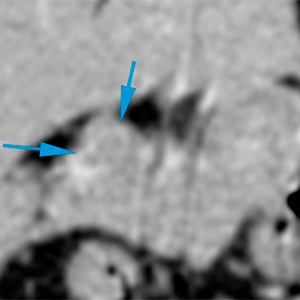
There are multiple filling defects with mineral foci along the gastroduodenal vein (orange arrows). In the cranial aspect of the mass, this vessel seems to be embedded within the mass with a filling defect, with possible invasion by the mass (blue arrows).
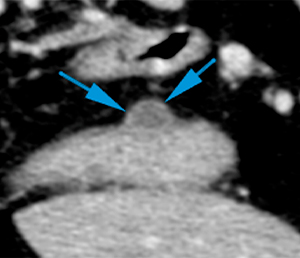
There is a small nodular lesion in the lesser curvature of the gastric body that shows mild homogeneous contrast enhancement. This lesion seems to originate in the serosal or muscular layer of the gastric wall with an eccentric growth (blue arrows).
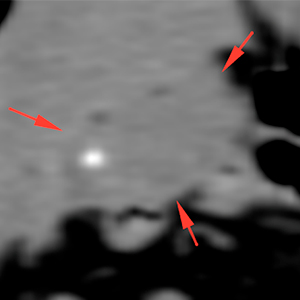
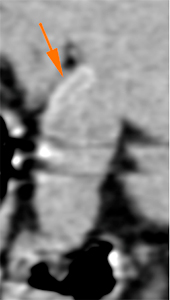
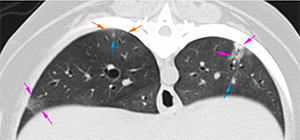
Thorax:There are multifocal areas of increased attenuation, with ill-defined and irregular margins, especially at the caudal lung lobes. Some of them have a peribronchial location (pink arrows) and others (orange arrow) are adjacent to ill-defined nodular lesions (blue arrow).
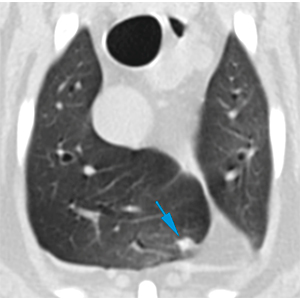
There are two irregular soft-tissue nodular lesions at the ventral and cranial aspects of the right cranial lung lobe (blue arrows).
Diagnosis
Abdomen:
Mass in the right pancreatic lobe, most likely consistent with neoplasia – neuroendocrine tumor (insulinoma) given the patient’s clinical signs and enhancement of the mass in the arterial phase -. Other neoplasia, such as adenocarcinoma, are also possible.
Possible vascular invasion and associated thrombus in the gastroduodenal vein before its insertion into the portal vein.
Gastric wall nodule (of serosal/muscular layer origin most likely), most likely consistent with neoplastic process – benign nodule like leiomyoma – or other benign lesions like cyst or granuloma. Malignant neoplasia is less likely.
Thorax:
Ill-defined nodular lesions that can be consistent with metastatic disease. Other ddx, such as an inflammatory/infectious process, are less likely.
Comments
Ultrasound-guided sampling of the pancreatic lesion is recommended. Thoracic CT-scan is recommended to monitor the progression of the ill-defined nodular lesions of the thoracic cavity.
(Mon. to Fri. 9 a.m. to 6 p.m. gmt+1) Welcome, How can we help you?
We use cookies to ensure that we give you the best experience on our website. If you continue to use this site we will assume that you are happy with it.Ok



No comment yet, add your voice below!