2-year-old male DSH with pleural effusion (chylothorax). Echocardiography did not reveal any abnormalities. An CT of the thorax was performed.
A thoracolumbar spine and thoracic CT scan was performed.
Description
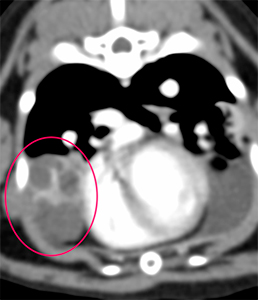
The right middle lung lobe shows an abrupt loss of visualization of the lobar bronchus close to its origin (pink arrows), followed by a lobar mass-like round lesion, with cavitary appearance and intralesional soft tissue septations (pink circles). Only these septations show contrast enhancement.
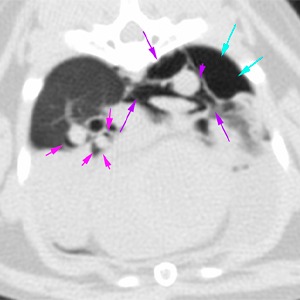
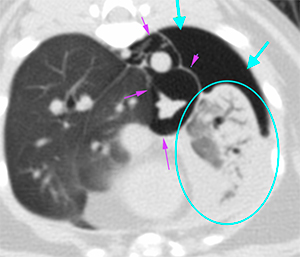
There is a mild amount of gas present in the interstitial space surrounding the primary pulmonary vessels of the right caudal and accessory lung lobes (pink arrows). A moderate amount of gas is observed localized in the mediastinum (purple arrows) and in the pleural cavity at the caudodorsal aspect of the left hemithorax (blue arrows). There is a moderate amount of pleural effusion occupying the ventral region of the left hemithorax (orange arrows).
There is a moderated retraction of the lung fields with presence of air bronchograms at the left cranial and caudal lung lobes with homogeneous enhancement after contrast administration (blue circle).
The sternal lymph nodes are slightly enlarged.
Diagnosis
Cavitary lobar lesion with abrupt loss of visualization of the lobar bronchus of the right middle lung lobe suggestive of lung lobe torsion; primary pathology such as lung abscess or cystic neoplasm, less likely, cannot be ruled out as a predisposing factor to lung torsion.
Interstitial emphysema with perivascular distribution affecting the right caudal and accessory lung lobes, consistent with Mackling effect (alveolar rupture due to the lesion described above).
Secondary pneumothorax, pneumomediastinum and left pleural effusion with atelectasis in the left lung lobes.
Mild sternal lymphadenopathy: reactive vs metastasis
Comments
The study shows a lesion suggestive of lung lobe torsion with associated pleural effusion (chylothorax according to the clinical history), with interstitial emphysema, pneumomediastinum and pneumothorax. The origin of these changes is uncertain, but it is suspected that the lung injury may have led to pulmonary interstitial emphysema that progressed to pneumomediastinum and pneumothorax. However, another origin cannot be ruled out and it should be assessed whether thoracentesis has been previously performed. Ultrasonography of the right middle lung lobe is recommended. Surgery and sampling of the cavitary lesion is recommended in order to reach a definitive diagnosis.
(Mon. to Fri. 9 a.m. to 6 p.m. gmt+1) Welcome, How can we help you?
We use cookies to ensure that we give you the best experience on our website. If you continue to use this site we will assume that you are happy with it.Ok







No comment yet, add your voice below!