8-year-old female neutered crossbreed. History of progressive loss of mobility in the hindlimbs. Came to the emergency room with paraparesis and loss of deep pain perception.
A thoracolumbar spine and thoracic CT scan was performed.
Description
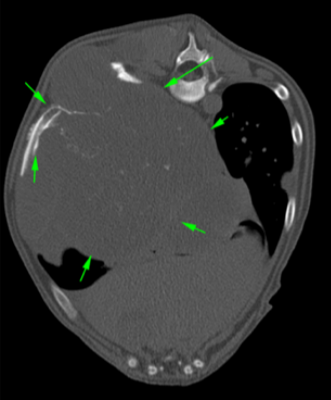
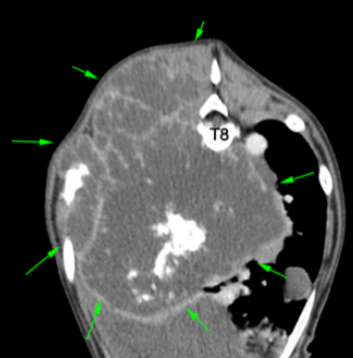
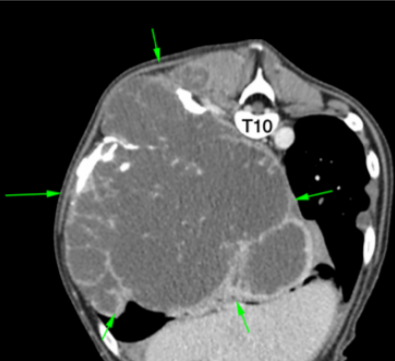
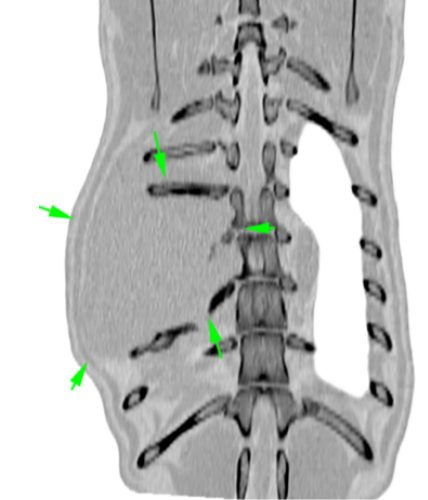
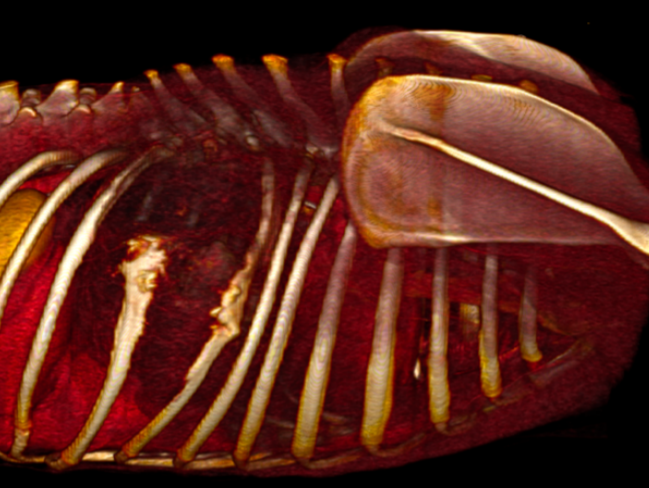
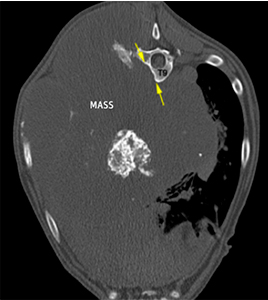
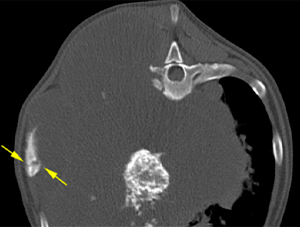
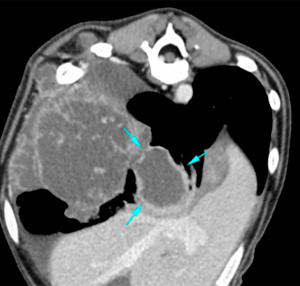
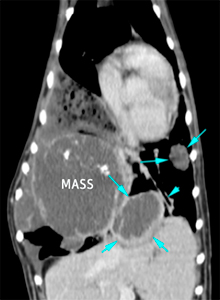
There is a large mass originating from the dorsal aspect of the 9th rib of the right costal wall, with separation of this rib from the adjacent ones. The mass is osteolytic, hypoattenuating with intralesional mineralisation and shows heterogeneous and mild post-contrast enhancement (green arrows). It severely invades the thoracic cavity producing a mass effect with displacement of the mediastinum towards the left and the rest of the pulmonary lobes, as well as the diaphragm caudally. It also invades the intercostal and paravertebral musculature in the area bulging outside, and produces lysis by compression of the ventral aspect of the vertebral bodies of T8 and T9, without evidence of invasion of the vertebral canal (yellow arrows). There is also a moderate irregular periosteal reaction, as well as a fracture line in the middle aspect of the 8th rib (yellow arrows).
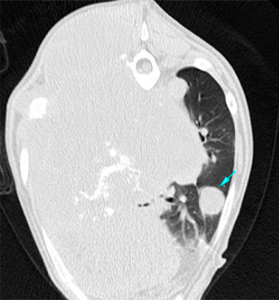
The lung parenchyma presents multiple, variable in size, hypoattenuating nodules, with a hyperattenuating and irregular wall, with the largest nodule located in the right caudal lung lobe (2.5-6cm) (blue arrows).
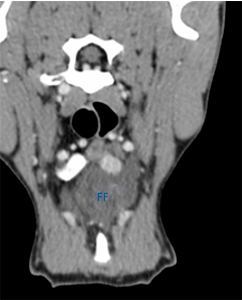
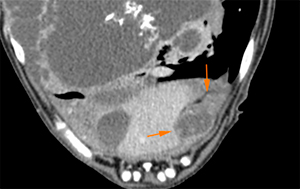
Moderate amount of hypoattenuating pleural fluid (FF). Irregular thickening of the parietal pleura forming nodular lesions with heterogeneous enhancement, mostly at the caudoventral aspect of the thoracic cavity (orange arrows).
Prominent sternal lymph nodes, with homogeneous contrast enhancement.
Diagnosis
Mass at the right costal wall originating from the 9th rib and affecting the 8th and 10th ribs, vertebral bodies and musculature consistent with a neoplastic process (i.e. osteosarcoma, chondrosarcoma, haemangiosarcoma).
Pulmonary nodules compatible with pulmonary metastases.
Pleural thickening and nodules consistent with metastases.
Pleural effusion.
Sternal lymphadenopathy, most likely metastatic vs reactive.
Comments
Sampling of the mass is recommended in order to reach a definitive diagnosis.
(Mon. to Fri. 9 a.m. to 6 p.m. gmt+1) Welcome, How can we help you?
We use cookies to ensure that we give you the best experience on our website. If you continue to use this site we will assume that you are happy with it.Ok


No comment yet, add your voice below!