6-years-old, male, DSH cat with chronic coughing, FIV positive. Alveolar lung pattern in ventral lung areas was seen on X-rays. A thoracic CT-scan was performed.
Description
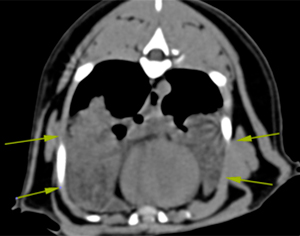
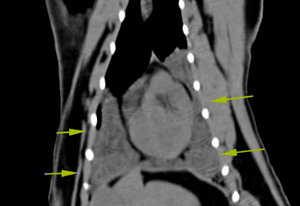
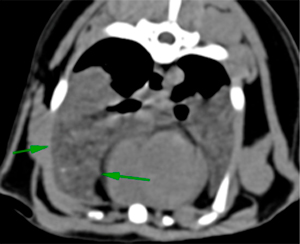
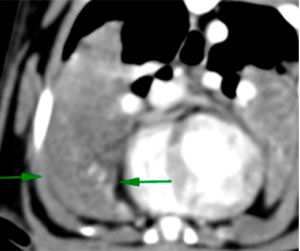
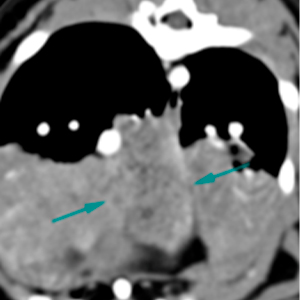
The lung parenchyma is not well aerated. There is a marked increase in attenuation and consolidation in the dependent regions of all the lung lobes, with presence of air bronchograms, while preserving a normal volume (yellow arrows). These changes are more marked in the right middle and accessory lung lobes (green and blue arrows respectively). In these two lobes, the parenchyma has heterogeneous appearance (reticulated alveolar pattern) with moderate heterogeneous contrast enhancement. The rest of the lung lobes show homogeneous enhancement.
Pre-contrast
Post-contrast
Pre-contrast
Post-contrast
Pre-contrast
Post-contrast
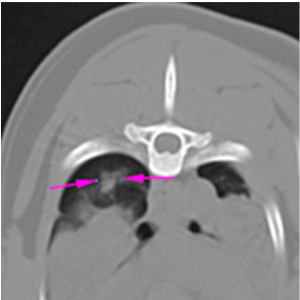
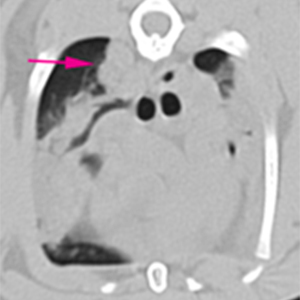
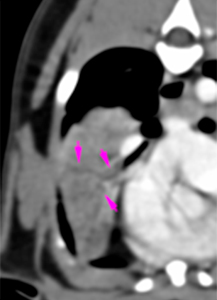
At the dorsal aspect of the right cranial and right caudal lung lobes, there are multiple (at least 3), variable in size, nodular lesions (pink arrows). Some of them have ill-defined margins.
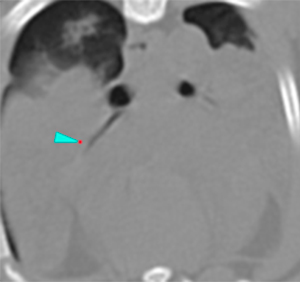
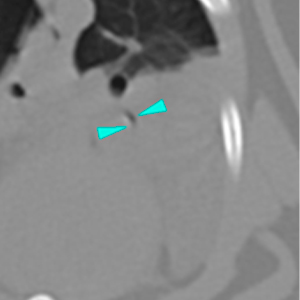
Some branches of the bronchi (third branches) show an abrupt ending (blue arrowheads), with the most distal portion of the bronchi having a lumen filled with fluid attenuating material (“fluid bronchogram”) (pink arrowheads).
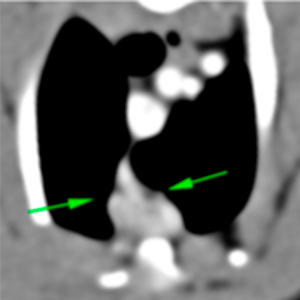
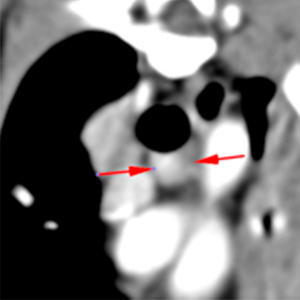
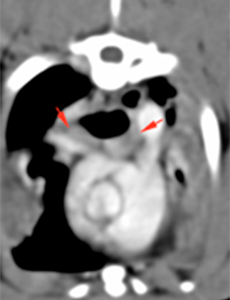
The sternal (green arrows), cranial mediastinal and tracheobronchial (red arrows) lymph nodes are slightly enlarged (5 mm), showing a slightly heterogeneous post-contrast enhancement.
Diagnosis
Multifocal alveolar lung pattern with ventral distribution throughout the lung fields. Differential diagnosis to consider include: inflammatory or infectious pneumonia (bacterial/viral origin- consider Mycoplasma spp. or tuberculosis, among others-; fungal or parasitic also possible, considering the severity and presence of concomitant lymphadenopathy); lipid pneumonia, cannot be ruled out; diffuse neoplasia (lymphoma or carcinoma) less likely.
Nodular lesions in the dorsal regions of the right cranial and caudal lung lobes: granulomatous process (bacterial, parasitic, or fungal), most likely associated with the previously described pneumonic process. Other differentials, such as neoplastic process, are considered less likely.
Thoracic lymphadenopathy, most likely reactive.
Comments
Follow up: In the bronchoalveolar lavage, a Mycoplasmaspp was cultured. Lung biopsies (right middle lung lobe) were performed by thoracoscopy, where histopathology diagnosed severe, chronic-active, generalized lipid pneumonia with multiple granulomas around necrotic material, lipid vacuoles and cholesterol crystals.
Lipid pneumonia is defined as a type of irritant pneumonia characterised by pulmonary consolidations secondary to lipid accumulation, often within macrophages. It is classified, based on the origin of the lipid, as exogenous or endogenous. The exogenous type is due to aspiration of mineral oil preparations (treatment for constipation or other GI disorders, treatment of hairballs…). The endogenous type is usually the result of a lesion in the pneumocytes associated with an obstructive pulmonary disease (inflammatory, irritative, neoplastic…). In human medicine, some patients (a minority) have underlying disorders of lipid storage or metabolism characterised by a high serum lipid concentration and lipid deposition in organs, including the lungs; it may also have an idiopathic origin.
(Mon. to Fri. 9 a.m. to 6 p.m. gmt+1) Welcome, How can we help you?
We use cookies to ensure that we give you the best experience on our website. If you continue to use this site we will assume that you are happy with it.Ok





No comment yet, add your voice below!